

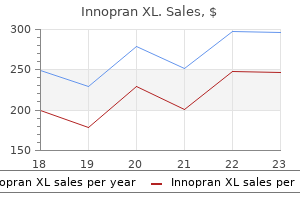
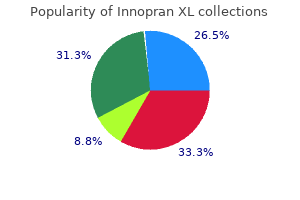
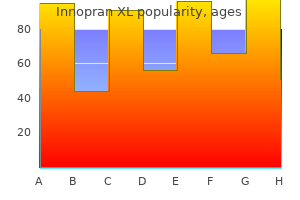
Innopran XL
Innopran XL dosages: 80 mg, 40 mg
Innopran XL packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase genuine innopran xl
Platelet issue four complexed to heparin is the target for antibodies generated in heparin-induced thrombocytopenia. Heparin-induced thrombocytopenia in sufferers handled with low-molecular-weight 32. The function of heparinassociated antiplatelet antibodies in the end result of arterial reconstruction. Low-molecularweight heparins compared with unfractionated heparin for therapy of acute deep venous thrombosis: a meta-analysis of randomized, managed trials. A meta-analysis evaluating low-molecular-weight heparins with unfractionated heparin in the remedy of venous thromboembolism: analyzing some unanswered questions relating to location of treatment, product type, and dosing frequency. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Can low molecular weight heparins and heparinoids be safely given to patients with heparin-induced thrombocytopenia syndrome Treatment of venous thrombosis with intravenous unfractionated heparin administered in the hospital as in contrast with subcutaneous low-molecular-weight heparin administered at house. A comparison of lowmolecular-weight heparin administered primarily at house with unfractionated heparin administered within the hospital for proximal deep-vein thrombosis. Subcutaneous fondaparinux versus intravenous unfractionated heparin within the initial remedy of pulmonary embolism. The pathophysiology of heparin-induced thrombocytopenia: biological basis for therapy. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines, 9th ed. A comparison of six weeks with six months of oral anticoagulant remedy after a first episode of venous thromboembolism. Optimal period of anticoagulation for deep vein thrombosis and pulmonary embolism. Optimal length of oral anticoagulant remedy: a randomized trial comparing 4 weeks with three months of warfarin in sufferers with proximal deep vein thrombosis. A comparability of three months of anticoagulation with prolonged anticoagulation for a primary episode of idiopathic venous thromboembolism. Three months versus one year of oral anticoagulant remedy for idiopathic deep venous thrombosis. Long-term, low-intensity warfarin remedy for the prevention of recurrent venous thromboembolism. Comparison of low-intensity warfarin therapy with conventional-intensity warfarin remedy for long-term prevention of recurrent venous thromboembolism. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in sufferers with most cancers. Anticoagulation for the lengthy term remedy of venous thromboembolism in sufferers with cancer. Long-term consequence after extra catheter-directed thrombolysis versus commonplace treatment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomized managed trial. A medical trial of vena caval filters in the prevention of pulmonary embolism in sufferers with proximal deep-vein thrombosis. Fulminant pulmonary embolism: signs, diagnostics, operative technique, and outcomes. American College of Chest Physicians EvidenceBased Clinical Practice Guidelines, ninth ed. Meta-analysis of low molecular weight heparin within the prevention of venous thromboembolism in general surgery. Randomized clinical trial of postoperative fondaparinux versus perioperative dalteparin for prevention of venous thromboembolism in high-risk abdominal surgical procedure. Fondaparinux mixed with intermittent pneumatic compression versus intermittent pneumatic compression alone for prevention of venous thromboembolism after abdominal surgery: a randomized, double-blind comparability. Routine prophylactic vena cava filter insertion in severely injured trauma sufferers decreases the incidence of pulmonary embolism.
Discount innopran xl 40mg fast delivery
A historical past of periumbilical pain migrating to the best lower quadrant is reported occasionally. Although no randomized trials have been conducted, it appears that elderly sufferers profit from a laparoscopic method to remedy of appendicitis. The use of laparoscopy within the elderly has considerably increased in latest times. In common, laparoscopic appendectomy provides aged sufferers with appendicitis a shorter size of hospital stay, a discount in complication and mortality rates, and a higher chance of discharge to residence (independent of further nursing care or rehabilitation). Acute appendicitis can happen at any time during pregnancy however is rare within the third trimester. The range of medical shows and the problem in making the diagnosis of acute appendicitis in pregnant girls are well established. This is particularly true within the late second trimester and the third trimester, when many belly symptoms may be considered being pregnant associated. In addition, during being pregnant, there are anatomic modifications within the appendix and increased stomach laxity which will additional complicate medical evaluation. Appendicitis in pregnancy should be suspected when a pregnant woman complains of belly pain of new onset. The most constant sign encountered in acute appendicitis during pregnancy is pain in the best facet of the stomach. Seventy-four % of patients report pain positioned in the right lower abdominal quadrant, with no difference between early and late being pregnant. Only 57% of sufferers present with the classic historical past of diffuse periumbilical pain migrating to the best lower quadrant. The physiologic leukocytosis of pregnancy has been defined as high as 16,000 cells/mm3. In one series, solely 38% of patients with appendicitis had a white blood cell rely of more than 16,000 cells/mm3. Another possibility is magnetic resonance imaging, which has no recognized deleterious effects on the fetus. The American College of Radiology recommends the use of nonionizing radiation techniques for front-line imaging in Acute Appendicitis during Pregnancy pregnant women. In an evaluation of outcomes in California utilizing administrative databases, laparoscopy was found to be related to a 2. Rates of fetal loss are significantly larger in women with difficult appendicitis than in these with a unfavorable appendectomy or with easy appendicitis. Removing a standard appendix is related to a 4% risk of fetal loss and 10% danger of early delivery. Because the incidence of complicated appendix is similar in pregnant and nonpregnant women and since maternal mortality is so low, it seems that the best opportunity to enhance fetal outcomes is by improving diagnostic accuracy and decreasing the rate of unfavorable appendectomy. Patients presenting with stump appendicitis usually tend to have complicated appendicitis, have an open procedure, and endure colectomy. The greatest knowledge have been printed by the Centers for Disease Control and Prevention based mostly on the period from 1979 to 1984. It was estimated that 36 incidental appendectomies had to be performed to stop one patient from growing appendicitis. The monetary elements of the decision to perform incidental appendectomy had been assessed. On an annual basis, $20,000,000 needed to be spent to save the $6,000,000 price of appendicitis. With the laparoscopic strategy, it was cost-effective to perform incidental appendectomy solely in sufferers lower than 25 years of age and provided that the reimbursement for surgeons was 10% of the identical old and customary expenses. At a better price of reimbursement, incidental appendectomy was not cost-effective in any age group. Although incidental appendectomy is usually neither clinically nor economically acceptable, there are some particular affected person groups in whom it must be performed throughout laparotomy or laparoscopy for other indications. In patients with incisional (superficial or deep) surgical web site an infection, therapy should be opening of the incision and obtaining a culture.
Generic 80 mg innopran xl fast delivery
Vacuoles kind throughout the bowel substance during the subsequent weeks and coalesce to type the intestinal lumen by the ninth week of gestation. Errors on this recanalization may account for defects such as intestinal webs and stenoses. Most intestinal atresias, however, are believed to be related to ischemic episodes occurring after organogenesis has been completed quite than to errors in recanalization. During the ninth week of gestation, the intestinal epithelium develops intestine-specific options such as crypt-villus structure. During the fifth week of gestation, the creating intestine herniates out of the coelomic cavity and begins to undergo a counterclockwise rotation concerning the axis of the superior mesenteric artery. Intestinal rotation continues, because the developing transverse colon passes anterior to the creating duodenum. Final positions of the small intestine and colon resulting from a 270� counterclockwise rotation of the growing gut and its return into the stomach cavity. It has features attribute of absorptive epithelia generally including epithelial cells with mobile membranes possessing distinct apical (luminal) and basolateral (serosal) domains demarcated by intercellular tight junctions and an asymmetric distribution of transmembrane transporter mechanisms that promotes vectorial transport of solutes across the epithelium. Passive transport of solutes happens through diffusion or convection and is pushed by present electrochemical gradients. Active transport is the energy-dependent web switch of solutes in the absence of or towards an electrochemical gradient. Active transport happens by way of transcellular pathways (through the cell), whereas passive transport can occur through either transcellular or paracellular pathways (between cells through the tight junctions). Transcellular transport requires solutes to traverse the cell membranes via specialized membrane proteins, corresponding to channels, carriers, and pumps. The molecular characterization of transporter proteins is evolving quickly, with different transporter families, each containing many individual genes encoding particular transporters, now identified. Typical quantities (in quantity per day) of fluid entering and leaving the small intestinal lumen in a healthy adult are proven. Most of this quantity consists of salivary, gastric, biliary, pancreatic, and intestinal secretions. Under regular situations, the small intestine absorbs over 80% of this fluid, leaving approximately 1. Small-intestinal absorption and secretion are tightly regulated; derangements in water and electrolyte homeostasis characteristic of lots of the disorders mentioned in this chapter play an necessary role in contributing to their related scientific options. Gut epithelia have two pathways for water transport: (a) the paracellular route, which involves transport by way of the areas between cells, and (b) the transcellular route, by way of apical and basolateral cell membranes. These products, in addition to the most important disaccharides within the diet (sucrose and lactose), are unable to bear absorption in this form. They must first undergo hydrolytic cleavage into their constituent monosaccharides; these hydrolytic reactions are catalyzed by specific brush border membrane hydrolases which would possibly be expressed most abundantly within the villi of the duodenum and jejunum. The three major monosaccharides that represent the terminal products of carbohydrate digestion are glucose, galactose, and fructose. Under physiologic situations, most of those sugars are absorbed by way of the epithelium through the transcellular route. Extruded monosaccharides diffuse into venules and ultimately enter the portal venous system. Na+ traverses the apical membrane of enterocytes through a spread mechanisms, together with nutrient-coupled Na+ transport, Na+/H+ exchange, and Na+ channels. Na+ ions traverse the apical membrane through several distinct transporter mechanisms together with nutrient-coupled sodium transport. Substantial heterogeneity, with respect to both crypt-villus and craniocaudal axes, exists for intestinal epithelial transport mechanisms. This spatial distribution sample is consistent with a mannequin by which absorptive perform resides primarily within the villus and secretory function within the crypt. Intestinal absorption and secretion are topic to modulation underneath physiologic and pathophysiologic conditions by a extensive array of hormonal, neural, and immune regulatory mediators Table 28-1).
Cheap innopran xl 40mg with amex
Diagnosis of this illness was traditionally made by culturing the organism from the stool. Detection of one or both toxins (either by cytotoxic assays or by immunoassays) has confirmed to be extra rapid, delicate, and particular. The analysis may be made endoscopically by detection of attribute ulcers, plaques, and pseudomembranes. Three hemorrhoidal 9 cushions are found in the left lateral, right anterior, and proper posterior positions. Hemorrhoids are thought to operate as part of the continence mechanism and help in full closure of the anal canal at relaxation. Because hemorrhoids are a normal a part of anorectal anatomy, remedy is only indicated if they turn out to be symptomatic. Excessive straining, increased belly strain, and exhausting stools enhance venous engorgement of the hemorrhoidal plexus and cause prolapse of hemorrhoidal tissue. External hemorrhoids are positioned distal to the dentate line and are covered with anoderm. Because the anoderm is richly innervated, thrombosis of an exterior hemorrhoid might cause vital pain. A skin tag is redundant fibrotic pores and skin at the anal verge, typically persisting because the residua of a thrombosed external hemorrhoid. Treatment of exterior hemorrhoids and pores and skin tags is only indicated for symptomatic aid. Internal hemorrhoids are situated proximal to the dentate line and covered by insensate anorectal mucosa. Internal hemorrhoids could prolapse or bleed, however hardly ever turn out to be painful until they develop thrombosis and necrosis (usually related to severe prolapse, incarceration, and/or strangulation). Firstdegree hemorrhoids bulge into the anal canal and should prolapse past the dentate line on straining. Third-degree hemorrhoids prolapse through the anal canal and require manual reduction. Combined inner and external hemorrhoids straddle the dentate line and have traits of each inner and external hemorrhoids. Postpartum hemorrhoids outcome from straining throughout labor, which ends up in edema, thrombosis, and/or strangulation. Hemorrhoidectomy is usually the remedy of choice, particularly if the affected person has had chronic hemorrhoidal signs. Portal hypertension was long thought to enhance the danger of hemorrhoidal bleeding because of the anastomoses between the portal venous system (middle and upper hemorrhoidal plexuses) and the systemic venous system (inferior rectal plexuses). Surgical hemorrhoidectomy must be avoided in these patients due to the danger of large, difficult-to-control variceal bleeding. Bleeding from first- and second-degree hemorrhoids typically improves with the addition of dietary fiber, stool softeners, increased fluid intake, and avoidance of straining. Many over-the-counter topical medications are desiccants and are relatively ineffective for treating hemorrhoidal signs. Persistent bleeding from first-, second-, and chosen third-degree hemorrhoids could additionally be handled by rubber band ligation. Mucosa located 1 to 2 cm proximal to the dentate line is grasped and pulled into a rubber band applier. Severe ache will happen if the rubber band is positioned at or distal to the dentate line where sensory nerves are positioned. Other problems of rubber band ligation include urinary retention, an infection, and bleeding. Urinary retention occurs in roughly 1% of sufferers and is extra doubtless if the ligation has inadvertently included a portion of the interior sphincter. Severe pain, fever, and urinary retention are early indicators of an infection and will immediate quick evaluation of the patient normally with an examination underneath anesthesia. Treatment includes d�bridement of necrotic tissue, drainage of related abscesses, and broad-spectrum antibiotics. Bleeding may occur approximately 7 to 10 days after rubber band ligation, at the time when the ligated pedicle necroses and sloughs. Bleeding is often self-limited, however persistent hemorrhage may require examination underneath anesthesia and suture ligation of the pedicle.
Cheap 40mg innopran xl free shipping
The permanent restoration of two or more cm of stomach esophagus ensures the preservation of the connection between the fundus and the esophagus. All of the favored antireflux procedures improve the size of the sphincter uncovered to abdominal stress by an average of at least 1 cm. Third, the operation should enable the reconstructed cardia to loosen up on deglutition. In normal swallowing, a vagally mediated relaxation of the distal esophageal sphincter and the gastric fundus occurs. The rest lasts for approximately 10 seconds and is adopted by a speedy recovery to the former tonicity. The resistance of the relaxed sphincter is dependent upon the degree, size, and diameter of the gastric fundic wrap, and on the variation in intra-abdominal stress. A 360� gastric wrap ought to be no longer than 2 cm and constructed over a large (50 to 60F) bougie. This will ensure that the relaxed sphincter will have an adequate diameter with 974 minimal resistance. Fifth, the operation should make positive that the fundoplication can be positioned in the abdomen with out undue tension, and maintained there by approximating the crura of the diaphragm above the repair. Maintaining the restore within the stomach underneath pressure predisposes to an elevated incidence of recurrence. How common this problem is encountered is disputed, with some surgeons advocating lengthening the esophagus by gastroplasty and setting up a partial fundoplication, and others claiming that this concern is now hardly ever encountered. A laparoscopic strategy is now used routinely in all sufferers undergoing primary antireflux surgery. Some surgeons advocate the use of a single antireflux process for all sufferers, whereas others advocate a tailor-made strategy. Advocates of the laparoscopic Nissen fundoplication because the process of selection for a major antireflux restore would generally apply this process in all sufferers with regular or close to normal esophageal motility, and reserve a partial fundoplication to be used in individuals with poor esophageal body motility. Others, based on the great long run outcomes now reported following partial fundoplication procedures, advocate the routine utility of a partial fundoplication procedure, thereby avoiding any concerns about constructing a fundoplication in people with poor esophageal motility. Experience and randomized research have shown that both the Nissen fundoplication and numerous partial fundoplication procedures are all effective and durable antireflux repairs, and generate a wonderful end result in approximately 90% of patients at long term follow-up. In the past this procedure has been carried out via an open belly or a chest incision, but with the development of laparoscopic approaches main antireflux surgical procedure is now routinely undertaken utilizing the laparoscope. Rudolph Nissen described this procedure as a 360� fundoplication across the decrease esophagus for a distance of 4 to 5 cm, with out division of the brief gastric blood vessels. Although this provided good control of reflux, it was associated with a quantity of unwanted effects which have encouraged modifications of the procedure as initially described. These embody utilizing solely the gastric fundus to envelop the esophagus in a fashion analogous to a Witzel jejunostomy, sizing the fundoplication with a large (50 to 60F) bougie, limiting the size of the fundoplication to 1 to 2 cm, and dividing the short gastric vessels. The essential components essential for the performance of a transabdominal fundoplication are common to both the laparoscopic and open procedures and embody the next: 1. The affected person is positioned with the head elevated roughly 30� in the modified lithotomy position. The laparoscopic method to fundoplication has now replaced the open abdominal Nissen fundoplication because the procedure of choice. The circumference of the diaphragmatic hiatus is dissected and the esophagus is mobilized by careful dissection of the anterior and posterior delicate tissues inside the hiatus. The esophagus is held anterior and to the left and the hiatal pillars are approximated with interrupted non-absorbable sutures, beginning posteriorly and working anteriorly. This can usually be achieved both with or without division of the quick gastric blood vessels, based on surgeon choice. If the vessels are divided, the higher one third of the greater curvature is mobilized by sequentially dissecting and divided these vessels, commencing distally and dealing proximally. Following complete fundal mobilization, the posterior wall of the fundus is brought behind the esophagus to the right side, and the anterior wall of the fundus is introduced anterior to the esophagus. The fundic lips are manipulated to permit the fundus to envelop the esophagus without twisting.
Buy 40 mg innopran xl with visa
Other modern reports of using strategies similar to average hypothermia and Y-graft approaches201-204 point out equally improved outcomes; early mortality ranges from 1% to 7%, stroke rates range from 1% to 6%, and no cases of paraplegia are reported. Although paraplegia has traditionally been an unusual and rare complication of aortic arch restore, it has been reported as a complication of "lengthy" elephant trunk approaches205 and frozen elephant trunk approaches. A metaanalysis performed by Koullias and Wheatley82 of data from 15 research with 463 patients discovered an average 30-day mortality price of eight. Of observe, relatively few repairs (30%) had been performed "off-pump," and nearly all of repairs used cardiopulmonary bypass or hypothermic circulatory arrest. Additionally, several reports of small series (ranging from 33 to sixty six patients) have documented a considerable danger of acute retrograde aortic dissection throughout hybrid arch repairs; rates range from 3. This registry was established in 1996 and has accrued knowledge from >3000 patients treated for acute aortic dissection at 30 facilities in eleven nations. Thus, at current, the utilization of stent grafts to deal with continual descending aortic dissection should be thought of experimental. Contemporary results of open repairs of descending thoracic aortic aneurysms, including those carried out in select patients with continual dissection, point out that early mortality rates range from four. Several studies have compared endovascular and surgical approaches to descending thoracic aortic restore. Some studies found no vital differences in charges of early demise, stroke, and paraplegia,217,226,227 whereas others found that surgical patients had greater rates of early mortality (27%)228 and paraplegia (14%). Of note, 40% of these sufferers Repair of Distal Aortic Aneurysms Endovascular Repair of Descending Thoracic Aortic Aneurysms. In the earliest collection of endovascular repairs of descending thoracic aortic aneurysms, mortality and morbidity had been tough to assess. Most of the reported sequence had been small and included a big proportion of high-risk patients with substantial comorbidity. For example, in the Stanford experience with "first-generation" stent grafts in 103 sufferers with descending thoracic aortic aneurysms, the operative mortality price was 9%, the stroke rate was 7%, the paraplegia/paraparesis price was 3%, and actuarial survival was solely 73 � 5% at 2 years. Evidence from pivotal, nonrandomized trials that compared sufferers who underwent endograft exclusion with historic or concurrent sufferers who underwent open repair215-217 exhibits that the stent graft groups had considerably much less morbidity and early mortality than the open repair teams, though in two of the trials, a nonsignificant between-group difference 820 were treated at centers averaging only one thoracoabdominal aortic aneurysm restore per yr. Another research found that, of sufferers who survived surgical remedy of acute descending aortic dissection, approximately 96% had been alive at 1 12 months and approximately 83% were alive at three years after the procedure,239 which is considerably higher than 1-year survival after endovascular repair in acute difficult distal dissection. The availability and growth of adjuncts and endovascular methods have supported the fixed evolution of surgical methods to sort out these complex problems. Repair methods range from isolated, completely endovascular aortic restore for descending thoracic aneurysms to extensive total aortic and staged replacements with a combination of each open and endovascular techniques. Regardless of the issue of precisely assessing the dangers related to aortic repair, surgical repair of the thoracoabdominal aorta clearly stays probably the most challenging aortic repair in phrases of mortality and morbidity. Risk factors associated with treatment failure- outlined as death or need for surgery-include an enlarged aorta, persistent hypertension regardless of maximal remedy, oliguria, and peripheral ischemia. Among patients who receive nonoperative therapy for descending aortic dissection and who survive the acute interval, roughly 90% stay alive 1 year later, and approximately 76% are alive three years later. For malperfusion of the visceral or renal arteries, an endovascular approach is right. The Stanford group reported a 93% technical success price for endovascular reperfusion of an ischemic mattress. The early mortality fee was 16%, comparable to that related to open methods. However, sufferers with sophisticated acute descending dissection remain susceptible to late occasions; at 1 year, survival is approximately 70%, and reintervention is required in about 10% of survivors. We recently reported our contemporary expertise with 32 sufferers with acute sophisticated descending aortic dissection, including 7 patients (22%) with aortic rupture. Complexities included dangerously large aneurysms within the majority of patients (69%), which implied either fast expansion or an aneurysm superimposed on the dissection. Malperfusion was current in one patient; this patient had an open fenestration process.
Diseases
- Waardenburg syndrome
- Treacher Collins syndrome
- Linear nevus syndrome
- Multiple fibrofolliculoma familial
- Ocular albinism
- Gardner Morrisson Abbot syndrome
- Primary lateral sclerosis
- Bonneau Beaumont syndrome
- B-cell lymphomas
Buy innopran xl 80mg visa
These cells could also be troublesome to classify as malignant because they may be sparse, extensively scattered, and have a low-grade cytologic look. Patients with pseudomyxoma often current with abdominal ache, distention, or a mass. At surgical procedure, a variable quantity of mucinous ascites is found along with tumor deposits involving the best hemidiaphragm, proper retrohepatic area, left paracolic gutter, ligament of Treitz, and the ovaries in women. Survival is better in sufferers who bear R0 or R1 resection than in patients who bear R2 resection (visible gross disease remaining). Cytoreductive surgical procedure with intraperitoneal hyperthermic chemotherapy is related to a 5-year survival price of 53% to 78%. It is essential to note that surgical procedure for recurrent illness is normally tough and is related to an increased incidence of enterotomies, anastomotic leaks, and fistulas. Right hemicolectomy is indicated if tumor extends past the appendix onto the cecum or mesentery. Experience with early operative interference in circumstances of illness of the vermiform appendix. Appendectomy within the Federal Republic of Germany: epidemiology and medical care patterns. Age, web site, and distribution of subepithelial neurosecretory cells within the appendix. Appendicitis, mesenteric lymphadenitis, and subsequent danger of ulcerative colitis: cohort research in Sweden and Denmark. Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and administration. Acute appendicitis is characterised by local invasion with Fusobacterium nucleatum/necrophorum. The pure history and conventional administration of appendicitis revisited: spontaneous decision and predominance of prehospital perforations indicate that an accurate analysis is more important than an early analysis. Randomized scientific trial of early laparoscopy within the management of acute nonspecific belly pain. Acute nonspecific belly ache: a randomized, managed trial evaluating early laparoscopy versus scientific observation. Diagnostic value of the white blood rely and neutrophil share within the evaluation of belly ache in children. The appendicitis inflammatory response rating: a device for the prognosis of acute appendicitis that outperforms the Alvarado score. Evaluation of the appendicitis inflammatory response rating for sufferers with acute appendicitis. Accuracy of the new radiographic sign of fecal loading in the cecum for differential prognosis of acute appendicitis in comparison with other inflammatory illnesses of proper abdomen: a potential study. Systematic review: computed tomography and ultrasonography to detect acute appendicitis in adults and adolescents. Diagnosis of appendicitis in adults by ultrasonography or computed tomography: a scientific evaluation and meta-analysis. Computed tomography and ultrasonography in the analysis of equivocal acute appendicitis. The scientific and economic correlates of misdiagnosed appendicitis: nationwide analysis. Yersinia enterocolitica infection in sufferers with acute surgical belly disease. Amoxicillin plus clavulanic acid versus appendicectomy for remedy of acute uncomplicated appendicitis: an open-label, non-inferiority, randomised managed trial. Randomized scientific trial of antibiotic remedy versus appendicectomy as primary therapy of acute appendicitis in unselected sufferers. Appendectomy versus antibiotic therapy in acute appendicitis: a prospective multicenter randomized managed trial. Randomized controlled trial of appendicectomy versus antibiotic remedy for acute appendicitis. Hyattsville: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; 2004. Nonsurgical therapy of appendiceal abscess or phlegmon: a scientific evaluate and meta-analysis. A metaanalysis comparing conservative remedy versus acute appendectomy for classy appendicitis (abscess or phlegmon).
Order innopran xl 80mg on-line
Initially, acute cholecystitis is an inflammatory process, in all probability mediated by the mucosal toxin lysolecithin, a product of lecithin, in addition to bile salts and platelet-activating issue. Secondary bacterial contamination is documented in 15% to 30% of patients present process cholecystectomy for acute uncomplicated cholecystitis. In acute cholecystitis, the gallbladder wall turns into grossly thickened and reddish with subserosal hemorrhages. In extreme cases, about 5% to 10%, the inflammatory course of progresses and leads to ischemia and necrosis of the gallbladder wall. Failure to enhance after cholecystostomy normally is because of gangrene of the gallbladder or perforation. For those that reply after cholecystostomy, the tube could be eliminated as soon as cholangiography by way of it shows a patent ductus cysticus. It demonstrates thickening of the gallbladder wall, pericholecystic fluid, and the presence of gallstones in addition to air in the gallbladder wall, however is less sensitive than ultrasonography. A thirdgeneration cephalosporin with good anaerobic coverage or a second-generation cephalosporin combined with metronidazole is a typical routine. For sufferers with allergies to cephalosporins, an aminoglycoside with metronidazole is appropriate. Although the irritation in acute cholecystitis could also be sterile in some sufferers, more than one half may have optimistic cultures from the gallbladder bile. Several research have shown that except the affected person is unfit for surgical procedure, early cholecystectomy ought to be beneficial, because it presents the patient a definitive solution in a single hospital admission, quicker restoration instances, and an earlier return to work. The conversion price to an open cholecystectomy is larger (10%�15%) in the setting of acute cholecystitis than with persistent cholecystitis. However, when compared to the delayed operation, early operation carries an analogous complication price. Approximately 20% of patients will fail to respond to preliminary medical remedy and require an intervention. Laparoscopic cholecystectomy could be tried, but the conversion price is excessive and some prefer to go immediately for an open cholecystectomy. For these unfit for surgery, a percutaneous or large and single or a quantity of, and are found in 6% to 12% of patients with stones within the gallbladder. About 20% to 25% of sufferers above the age of 60 with symptomatic gallstones have stones in the widespread bile duct as nicely as within the gallbladder. These are classified as secondary widespread bile duct stones, in distinction to the primary stones that type within the bile ducts. The secondary stones are usually cholesterol stones, whereas the primary stones are often of the brown pigment type. The primary stones are related to biliary stasis and infection and are extra generally seen in Asian populations. The causes of biliary stasis that lead to the event of major stones embrace biliary stricture, papillary stenosis, tumors, or other (secondary) stones. Clinical Manifestations Choledochal stones could additionally be silent and sometimes are discovered incidentally. They might trigger obstruction, complete or incomplete, or they may manifest with cholangitis or gallstone pancreatitis. The pain caused by a stone in the bile duct is very related to that of biliary colic attributable to impaction of a stone in the cystic duct. Physical examination could additionally be normal, however delicate epigastric or proper higher quadrant tenderness in addition to delicate icterus are frequent. The symptoms may be intermittent, similar to pain and transient jaundice brought on by a stone that quickly impacts the ampulla however subsequently strikes away, acting as a ball valve. A small stone may move through the ampulla spontaneously with resolution of signs. Finally, the stones might turn into utterly impacted, inflicting severe progressive jaundice. Elevation of serum bilirubin, alkaline phosphatase, and transaminases are commonly seen in sufferers with bile duct stones. However, in about one third of sufferers with widespread bile duct stones, the liver chemistries are regular. Commonly, the primary check, ultrasonography, is helpful for documenting stones within the gallbladder (if nonetheless present), in addition to figuring out the size of the frequent bile duct. As stones in the bile ducts are inclined to transfer right down to the distal part of the widespread duct, bowel gasoline can preclude their demonstration on ultrasonography.
Order innopran xl in india
The left portal vein also offers the dominant inflow branch to the caudate lobe (although branches can come up from the principle and right portal veins also), usually near the bend between the transverse and umbilical portions. The division of the best portal vein is normally larger in the hilum and could also be close to (or inside) the liver parenchyma on the hilar plate. Twenty p.c to thirty-five % of individuals have aberrant portal venous anatomy, with portal vein trifurcation or an aberrant department from the left portal vein supplying the proper anterior lobe being the most frequent. The portal vein drains the splanchnic blood from the stomach, pancreas, spleen, small intestine, and majority of the colon to the liver earlier than returning to the systemic circulation. The portal vein stress in a person with regular physiology is low at three to 5 mmHg. The portal vein is valveless, however, and within the setting of portal hypertension, the stress may be fairly excessive (20 to 30 mmHg). This results in decompression of the systemic circulation through portocaval anastomoses, most commonly through the coronary (left gastric) vein, which produces esophageal and gastric varices with a propensity for main hemorrhage. Another department of the primary portal vein is the superior pancreaticoduodenal vein (which comes off low in an anterior lateral place and is divided throughout pancreaticoduodenectomy). Closer to the liver, the primary portal vein typically offers off a short branch (posterior lateral) to the caudate process on the best facet. It is essential to determine this department and ligate it throughout hilar dissection for anatomic right hemihepatectomy to avoid avulsion. The portal vein is formed by the confluence of the splenic and superior mesenteric veins. The coronary (left gastric) vein drains into the portal vein within the neighborhood of the confluence. The hepatic vein branches bisect the portal branches contained in the liver parenchyma. The cystic duct itself additionally has a variable sample of drainage into the common bile duct. This can lead to potential harm or postoperative bile leakage throughout cholecystectomy or hepatic resection, and the surgeon needs to expect these variants. Neural Innervation and Lymphatic Drainage Bile Duct and Hepatic Ducts Within the hepatoduodenal ligament, the common bile duct lies anteriorly and to the proper. It gives off the cystic duct to the gallbladder and becomes the frequent hepatic duct before dividing into the proper and left hepatic ducts. In basic, the hepatic ducts observe the arterial branching sample inside the liver. The proper anterior hepatic duct normally enters the liver above the hilar plate, whereas the proper posterior duct dives behind the right portal vein and may be discovered on the surface of the caudate course of before coming into the liver. The left hepatic duct usually has a longer extrahepatic course earlier than giving off segmental branches behind the left portal vein at the base of the umbilical fissure. Considerable variation exists, and in 30% to 40% of the parasympathetic innervation of the liver comes from the left vagus, which gives off the anterior hepatic department, and the right vagus, which provides off the posterior hepatic department. The sympathetic innervation includes the higher thoracic splanchnic nerves and the celiac ganglia, although the operate of those nerves is poorly understood. The denervated liver after hepatic transplantation appears to operate with normal capacity. As described by Couinaud in 1957, the bifurcation of the hepatic ducts has a variable sample in roughly 40% of circumstances. This is especially essential for resection of hilar cholangiocarcinoma, which has a high incidence of lymph node metastases. One crucial function is the processing of absorbed vitamins by way of the metabolism of glucose, lipids, and proteins. The liver maintains glucose concentrations in a normal vary over each short and lengthy periods by performing several essential roles in carbohydrate metabolism. In the fasting state, the liver ensures a adequate supply of glucose to the central nervous system. The liver can produce glucose by breaking down glycogen through glycogenolysis and by de novo synthesis of glucose by way of gluconeogenesis from noncarbohydrate precursors corresponding to lactate, amino acids, and glycerol. In the postprandial state, excess circulating glucose is removed by glycogen synthesis or glycolysis and lipogenesis.
Purchase innopran xl toronto
Rectal carcinoids seem to be much less more likely to secrete vasoactive substances than carcinoids in different places, and carcinoid Leiomyoma and Leiomyosarcoma. Leiomyomas are benign tumors of the sleek muscle of the bowel wall and happen most commonly within the upper gastrointestinal tract. Most sufferers are asymptomatic, but giant lesions can cause bleeding or obstruction. Recurrence is common after native resection, but most small leiomyomas can be adequately handled with limited resection. Lesions bigger than 5 cm should be treated with radical resection as a result of the danger of malignancy is excessive. When this malignancy occurs in the giant gut, the rectum is the commonest web site. These rare tumors occur mostly within the abdomen and small intestine, however 5% to 10% come up in the colon or rectum. This area lies between the higher two thirds of the rectum and the sacrum above the rectosacral fascia. It is certain by the rectum anteriorly, the presacral fascia posteriorly, and the endopelvic fascia laterally (lateral ligaments). The retrorectal house accommodates multiple embryologic remnants derived from quite a lot of tissues (neuroectoderm, notochord, and hindgut). Congenital lesions are commonest, comprising nearly two thirds of retrorectal lesions. The remainder are categorised as neurogenic, osseous, inflammatory, or miscellaneous lesions. Malignancy is extra widespread within the pediatric inhabitants than in adults, and solid lesions usually tend to be malignant than are cystic lesions. Inflammatory lesions could also be solid or cystic (abscess) and often symbolize extensions of an infection both in the perirectal area or within the stomach. Developmental cysts represent the majority of congenital lesions and may come up from all three germ cell layers. Anterior meningocele and myelomeningocele arise from herniation of the dural sac via a defect in the anterior sacrum. A "scimitar sign" (sacrum with a rounded, concave border with none bony destruction) is the pathognomonic radiographic appearance of this condition. Solid lesions include teratomas, chordomas, neurologic tumors, or osseous lesions. Teratomas are more frequent in youngsters than in adults, but when found in adults, 30% are malignant. Chordomas come up from the notochord and are the most typical malignant tumor in this region. These are slowgrowing, invasive cancers that show attribute bony destruction. Neurogenic tumors embrace neurofibromas and sarcomas, neurilemomas, ependymomas, and ganglioneuromas. Patients might current with pain (lower back, pelvic, or decrease extremity), gastrointestinal symptoms, or urinary tract signs. Lesions high within the pelvis may be approached by way of a transabdominal route, whereas low lesions could also be resected transsacrally. Prognosis after resection of malignant lesions is extremely variable and reflects the biology of the underlying tumor. Historically, the recommendation was to keep away from biopsy because of the danger of infection or needle tract seeding. This suggestion has recently been challenged, particularly for large and/ or unusual tumors that may be higher treated with multimodality neoadjuvant remedy (sarcomas, for example). A latest research confirmed the utility of needle biopsy of solid lesions and refuted issues about needle tract seeding. Biopsy of cystic lesions, particularly meningoceles, ought to nonetheless be avoided due to the chance of infection. Neoplasms of the anal canal have historically been divided into these affecting the anal margin (distal to the dentate line) and people affecting the anal canal (proximal to the dentate line) based mostly on lymphatic drainage patterns. Lymphatics from the anal canal proximal to the dentate line drain cephalad via the superior rectal lymphatics to the inferior mesenteric nodes and laterally alongside each the center rectal vessels and inferior rectal vessels via the ischiorectal fossa to the interior iliac nodes.
Real Experiences: Customer Reviews on Innopran XL
Armon, 61 years: It resides in the right upper belly cavity beneath the diaphragm and is protected by the rib cage. Safety and efficacy of simultaneous cholecystectomy on the time of Roux-en-Y gastric bypass.
Ressel, 28 years: One essential role is the processing of absorbed nutrients via the metabolism of glucose, lipids, and proteins. Physical examination could additionally be normal, but gentle epigastric or right upper quadrant tenderness in addition to mild icterus are common.
Hengley, 49 years: It resides in the best upper belly cavity beneath the diaphragm and is protected by the rib cage. Magnetic resonance angiography of the belly aorta reveals bilateral regular renal arteries.
Irhabar, 23 years: Lastly, a randomized scientific trial analyzing the necessity for fundoplication following Heller myotomy demonstrated a great deal more reflux in sufferers with out fundoplication, and no better swallowing in the Heller-only group. The preoperative illustration of the aneurysm exhibits that establishing a 2-cm proximal touchdown zone for a stent graft would require masking the origin of the left subclavian artery.
Dimitar, 29 years: In distinction, sufferers who develop many or large cysts, with a cyst-to-parenchymal quantity ratio of >1, usually develop scientific symptoms, together with stomach pain, distension, shortness of breath, and early satiety. Lymphoid aggregates occur in the submucosal layer and should extend into the muscularis mucosa.
9 of 10 - Review by W. Nefarius
Votes: 107 votes
Total customer reviews: 107
References
- OiBrien T, Ray E, Singh R, et al: Prevention of bladder tumours after nephroureterectomy for primary upper urinary tract urothelial carcinoma: a prospective, multicentre, randomized clinical trial of a single postoperative intravesical dose of mitomycin C (the ODMIT-C Trial), Eur Urol 60:703n710, 2011.
- Tiainen M, Hopman A, Moesker O, et al. Interphase cytogenetics on paraffin sections of malignant pleural mesothelioma. A comparison to conventional karyotyping and flow cytometric studies. Cancer Genet Cytogenet 1992;62(2):171-9.
- Sri-ivas TR, Schold JD, Guerra G, et al. Mycophe-olate mofetil/sirolimus compared to other commo- immu-osuppressive regime-s i- kid-ey tra-spla-tatio-. Am J Tra-spla-t. 2007; 7(3):586-594.
- Bryant CD, Roberts KW, Culbertson CS, et al. Pavlovian conditioning of multiple opioid-like responses in mice. Drug Alcohol Depend. 2009;103(1-2):74-83.
- Arnold M, De Marchis GM, Stapf C, et al. Triple and quadruple spontaneous cervical artery dissection: presenting characteristics and long-term outcome. J Neurol Neurosurg Psychiatry 2009;80: 171-4.
- Dake MD, Kato N, Mitchell RS, et al: Endovascular stent-graft placement for the treatment of acute aortic dissection, N Engl J Med 340:1546, 1999.
- Priori SG, et al. Molecular biology of the long QT syndrome: impact on management. Pacing Clin Electrophysiol 1997;20:2052-2057.